


Why we haven't made breakthrough medical progress in the internet era, part 1: venture financing
They promised us cures for Alzheimer's, instead we got 145 cancer drugs

Why does it feel like we haven’t made significant medical progress in the internet era (1990-present)?
Significant medical breakthroughs were made throughout the 20th century. These breakthroughs added decades to human life expectancy either for acute/infectious diseases (e.g. penicillin in 1928) and chronic diseases (e.g. insulin and metformin for diabetes in the 1920’s, ACE inhibitors for high blood pressure in 1975, statins for high cholesterol / strokes in 1976), yet in the last few decades it appears we’ve hit a wall outside of a few more specific areas like antiretroviral therapies for HIV treatment/prevention in the mid-1990’s, cancer treatments in the last couple decades like Gleevec for CML and gastric cancers in 2001 and Keytruda for advanced cancer remission in 2014, and Sovaldi for curing Hepatitis C in 2007.

There are still a lot of large unsolved medical problems per ChatGPT: neurodegenerative diseases, cancer, antimicrobial resistance, chronic pain management, metabolic disorders, autoimmune diseases, rare genetic disorders, mental health disorders, and healthy aging / anti-aging among other emerging areas.
A few reasons why we’ve hit a wall in solving these problems:
The (venture) financing model for biology and drug discovery is broken
The clinical trials and FDA regulation regime is broken
Our understanding of biology, systems and diseases has not advanced
In this post I’ll outline the problems in the biotech venture financing model and some existing experiments and new ideas to address these problems.
The venture financing model is broken
To understand the biotech industry, you also have to understand how venture financing works. Venture capital (VC) investors (GPs or general partners) raise funds from institutional investors (LPs or limited partners, such as university endowments, pensions, sovereign wealth funds) with a fixed investment period (3 years) and horizon (10 years). VCs need to show evidence of returns about midway into their investment horizon in order to raise another fund, typically in the form of paper mark-ups on investments and initial portco exits via M&A and/or IPOs.
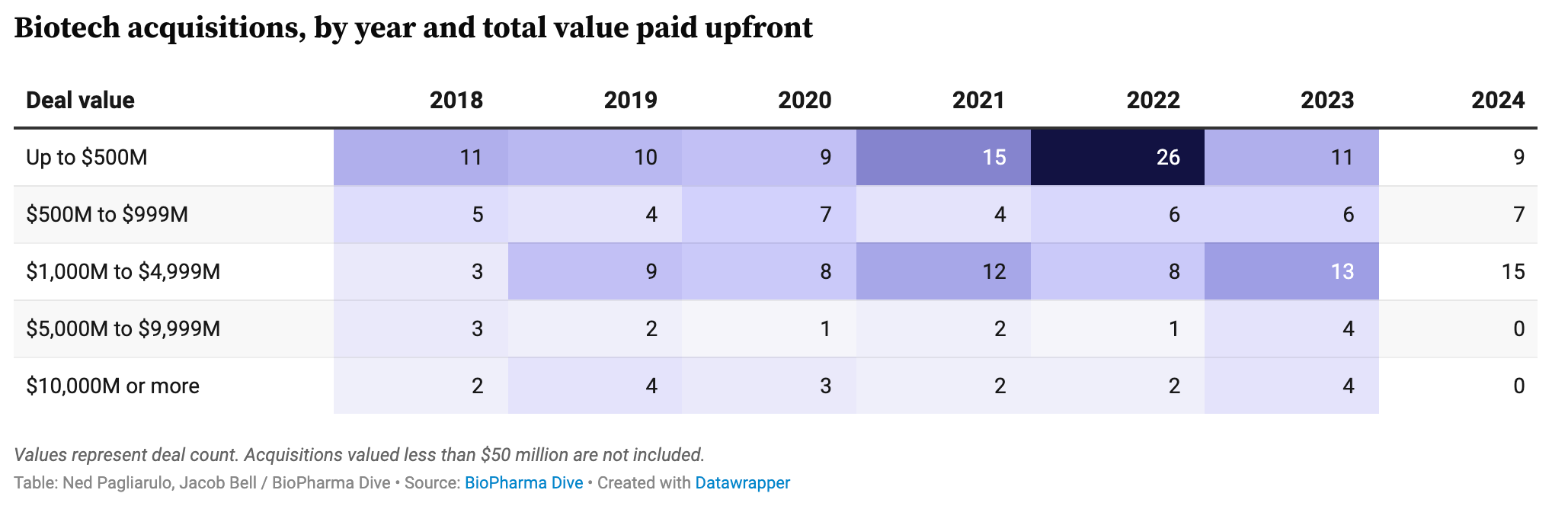
Venture funds are raising fewer funds, biotech IPOs and M&As on the decline
Venture capital (across industries) has been hammered as LPs are not doling out the money needed to support new funds as performance standards have risen and successful M&A and IPO outcomes are becoming rarer after a flurry of activity in 2021.


Outside of fewer successful outcomes and funds raised, founder dilution tends to be high (but maybe not as high as we may think per Sarah Hein’s deep dive) and biotech VCs have not been funding the bridge between drug discovery and clinical development. Per conversations with several preclinical biotech founders, it has been near impossible to fund human trials in a high interest rate environment outside of select best-in-class technologies.
Financing and business model experiments
There have been several experiments in the business model of financing biotech innovations over the last couple few decades, though it is hard to say any have helped shift the pace of medical breakthroughs yet:
Make large capital contributions to best in class tech + team (1986): ARCH & Bob Nelson. Biggest success to date is RNAi developer Alnylam with possibly the highest clinical trial success rate in the industry (60+% vs. 10% average) by using genetic evidence.
Bet on the most productive scientist entrepreneurs (1996): Polaris & Bob Langer (MIT), co-founder of 20 Polaris backed startups. Biggest success to date is also Alnylam, though not a Bob Langer founded company.
Place small bets in platform bio opportunities, encourage Darwinian competition via a rigorous process (2000): Flagship Pioneering. Biggest success is COVID mRNA vaccine darling Moderna
Hub & spoke clinical stage asset portfolio construction in line with Andrew Lo’s portfolio optimization theory (2009 /2014): Nimbus Therapeutics, Roivant, BridgeBio, and perhaps Formation Bio. Biggest success is likely in the autoimmune space with successful phase 2 readouts for Nimbus’s development of TYK2 inhibitor acquired by Takeda, and Roivant’s flip of potential best-in-class TL1A auto-immune candidate to Roche.
Get earlier liquidity via decentralized science funding and blockchain primitives (2021): Molecule with BioDAOs, IPNFTs, IPTs. Biggest success to date is tbd, but many bets on longevity via VitaDAO (disclosure: I’m an investor in Molecule and VitaDAO via Hydra).
Help startups get data to raise Series A with embedded fractional CSOs and a network of tier 1 LPs (2022): Curie Bio. Biggest success is tbd. Great overview of the model by Zach Weinberg here.
New ideas to try
Some new ideas to try to buck the challenges in biotech financing could include:
Financing disease understanding and data generation public goods infrastructure with focused research organizations (FROs). Focused research organizations are non-profits with focused goals and a finite time period to achieve those goals (~5-10 years). Some initial experiments along these lines include FutureHouse with the goal of building an AI scientist in the next 10 years by enabling better hypothesis generation, and E11 Bio with the goal of mapping the brain connectome starting with the mouse brain. This requires more LP / donor capital going into FROs, data partnerships, lab automation, top talent inflow from startups and academia, GPU compute accessibility (like Prime Intellect is starting to do, disclosure I’m an investor via Hydra).
Creating fully virtual drug discovery companies, where a founding team “in a garage” can flexibly scale multiple drug candidates into development at a lower cost. There are fewer examples to build on, but the closest is probably Nimbus Therapeutics (see CEO Jeb Keiper’s recounting of the Nimbus story). This requires investment in lab automation availability and capabilities, flexible access to contract drug manufacturing and research organizations (CDMOs and CROs), better AI/Ml discovery models, and clinical research partners with friendly licensing terms among other areas.
Create a Bob Langer (AI?) factory: Find the next Bob Langers out there, develop early partnerships with them and fund companies spun around their scientific ideas. Better yet create the AI Bob Langer and/or AI co-pilot to help talented scientists find new breakthrough scientific ideas. Maybe FutureHouse is trying to do this by creating an AI Scientist, but what if we created an ASI Scientist Entrepreneur (in this case ASI = artificial super-productive intelligence)? More innovations need to be made on the reasoning side of AI before this can happen, including linking ideas to potential clinical viability and financial traction.
Fund more drug repurposing (powered by AI?): Drug repurposing has the advantage of taking drugs that have been approved for one indication (and therefore proven safe in humans) and repurposing them for another indication. This can sometimes be like finding a needle in a haystack, but with LLMs maybe we can do this more effectively and efficiently like Every Cure is trying to do. There are a few successful examples of classic drug repurposing in recent years, as Trevor Klee outlined with breakdowns of Viking Therapeutics (GLP-1 acquired from Ligand, that outperformed Lilly GLP-1 leader Mounjaro) and Karuna Therapeutics (Alzheimer’s drug repurposed for schizophrenia and sold to BMS), though the journey can still take a decade plus.
Creating full stack drug discovery & development companies to lower unit economics of R&D. As described in a previous post, Vial is exploring this path with Battery Bio, reducing the cost per patient for clinical trials as a CRO for other pharma/biotech companies, while simultaneously using AI models to find drug candidates to go through these clinical trials. Less cost per drug candidate, means more shots on goal?
There are many more ideas to explore, and financing / business model structure is just one (tiny) hammer to fix the medical breakthroughs drought, though if any of you are pursuing anything around these new ideas please do reach out as I’d love to jam on these idea spaces further. Sometimes finance/business model innovation can help navigate the idea maze more efficiently.
As we will see in my next posts, there are larger problems and gaps in clinical trials and regulation, and our understanding of disease progression.