


Why we haven't made breakthrough medical progress in the internet era, part 3: our understanding of disease
We still can't beat chronic disease killers, and aging overall...yet

Hello to the 60+ new subscribers since my last post! For context, this post is the 3rd and last installment of a 3 part series exploring why we haven’t seen breakthrough medical progress in the last 30+ years since the internet has in parallel rapidly accelerated information technological progress:
The (venture) financing model for biology and drug discovery is broken
(this post) Our understanding of disease - its prevention, onset, progression, and reversal - is still very limited
Defining disease
Before we dive in, let’s first define what is a disease. It is 2024 so let’s ask ChatGPT:

As mentioned in my clinical trials post, the most correlated factors with clinical development success are modality (CAR-T, RNAi, mAb are winning strategies) and indication (hematology, cardio metabolic in the lead). The thing about human biology is that even if we fully understand the causes of disease, we have limited avenues to change its course. We are bound by the physical laws of the universe, specifically entropy. Treating the symptoms of disease, like reducing LDL cholesterol for atherosclerosis and heart disease, and beta-amyloid plaques & tau tangles for Alzheimer’s, can slow some progress, but just delays the inevitable course of progression despite some pleiotropic effects.
Disease trends in the US
While there have been breakthroughs in treatment of conditions that were once deemed early death life sentences (antiretroviral therapies like Truvada & Sunlenca for HIV prevention and maintenance treatment), and that are stubborn to impact by behavioral changes (GLP-1s like Wegovy and Mounjaro for obesity), we seem to have hit an asymptote in turning the tide on the biggest killers over the last few decades: heart disease and cancer. There was also a roughly tripling of absolute number of deaths from diabetes & COPD, and quadrupling in Alzheimer’s deaths.

Top drugs and lifespan + healthspan impact
Most commonly prescribed drugs for older adults (50+) are focused on heart disease prevention across high cholesterol, high blood pressure, later stage cardiovascular issues like heart failure, and diabetes. These medications have an impact on lifespan (statins especially with their pleiotropic effects) and healthspan, however don’t prevent death for very long as seen by this table:

Harnessing our immune systems and targeting the inflammasome
The most promising area for new breakthrough therapies is our immune system, our best defense system against the world and disease both acute and chronic. Our immune system can be reprogrammed to selectively attack cancerous cells (CAR-T therapeutics like Yescarta), dampened to prevent autoimmune symptoms (anti-TNF therapeutics like Humira), and more options we are not aware of yet. Keytruda, a PD-1 inhibitor therapeutic assisting the immune system in its fight against cancer, is projected to remain the top selling drug in the world through 2028 (already at $30B rate in 2024).
The next generation of therapeutics may focus on inflammation more broadly. Inflammation is theorized to be the root of most diseases. Persistent inflammation may lead to heart disease, diabetes, cancer and more life threatening diseases. Maybe repeated infections by viruses slowly wears down our defenses and makes us more susceptible to develop these chronic diseases. Targeting the “inflammasome” can potentially stem much of the harmful inflammation activity at the root of many diseases.

Defining normal and measuring our health (changes)
Going back to the definition of disease at the top of this post, there was something that we didn’t dive into: what is normal functioning of an organism, specifically humans?
The first step is understanding our genome. Improvements in the cost of (whole) genome sequencing and more prevalent testing can give us a better sense for what a normal human genome is and which mutations cause specific diseases.
Beyond genetics, we need to have measurement capabilities at a population scale. Existing measurements have varying levels of usage and accessibility:
vital sign measurements like heart rate / blood pressure / SpO2 among others (cheap, available on consumer electronics like Apple Watch / wearables)
blood tests (cheap, usually covered by insurance)
medical imaging (expensive, typically gated by insurance for inappropriate usage),
tissue samples (expensive, likely gated by insurance for specific symptom presentation)
invasive organ samples (expensive, gated by insurance for specific symptoms like cancer)
We have a sense of “normal”, but there are huge caveats:
Those lab reference values you receive on your blood test reports are based on a population sample that may include both “normal” and “diseased” individuals. According to Perplexity this reference setting exercise can include as many as 120 individuals, and ranges are set based on variation that covers 95% of the population and in some cases are just set on known risk factors (e.g. cholesterol and cardiovascular risk factors).
Radiologists are trained on interpreting normal medical images and deviations from them, but how do we know the individuals in the “normal” sample are actually normal or just very similar to each other? According to Gemini these are based on past cases and reference ranges, but once again there is some bias.
Why is any of this measurement important? These values can help us manage our health, diagnose disease and be used as inclusion criteria in clinical trials to see if a drug can change that value closer to or back in the reference range. Doctors know that the trend matters more than a static point, however reference ranges are important for risk stratification and treatment.
There are some companies trying to get a deeper sense of normal:
Verily, Project Baseline, studying what is normal
Function Health, 100+ lab tests for an annual fee
Ezra, full-body MRIs to catch early stage cancer
Longitudinal studies to better understand the transition from normal to diseased
Beyond static point measurements, longitudinal multi-year studies are very important to seeing how humans progress from normal to diseased states and what factors may cause these diseased states. Typically these studies will show correlation, and cannot establish causation, but areas of strong correlation can help narrow down areas of investigation for therapeutics and diagnostics.
Some government-sponsored longitudinal studies include:
The Framingham Heart Health study, running for 75+ years following 5K participants and the next generations giving insight into heart health drivers like exercise, statins
UK Biobank running for 18+ years on 500K participants, with blood/urine/saliva samples along with whole genome sequencing for some participants
All of Us (NIH) started in 2015 with a goal of 1M participants, currently at ~600K providing initial data
These studies have helped shape not only clinical guidance (exercise more, eat healthier), but also have been the direct / indirect source of drug discovery and development, particularly when looking at genetic testing. Longitudinal studies, with deep & frequent measurement are key to our understanding. How many more UK Biobanks and Framingham Heart Health studies can we create?
More studies will require industry and/or academic medical center sponsorship. There are several industry-sponsored longitudinal studies in partnership with academic medical centers such as NashBio, sponsored by many big pharma companies like GSK and facilitated by Vanderbilt University Medical Center to create BioVU a database of 11 years of 3.6M de-identified individuals’ health records matched with ~300K genetic samples. A predecessor to 23andMe, deCODE genetics, now owned by Amgen, has 2/3 of Iceland’s population participating in its studies. Genetic evidence is a key factor in improving the success rates of drugs, as seen by Alnylam’s industry-leading 62% end-to-end clinical development success rate for its largely RNAi therapeutics portfolio.
Aging as a final frontier, and the need for new scientific approaches
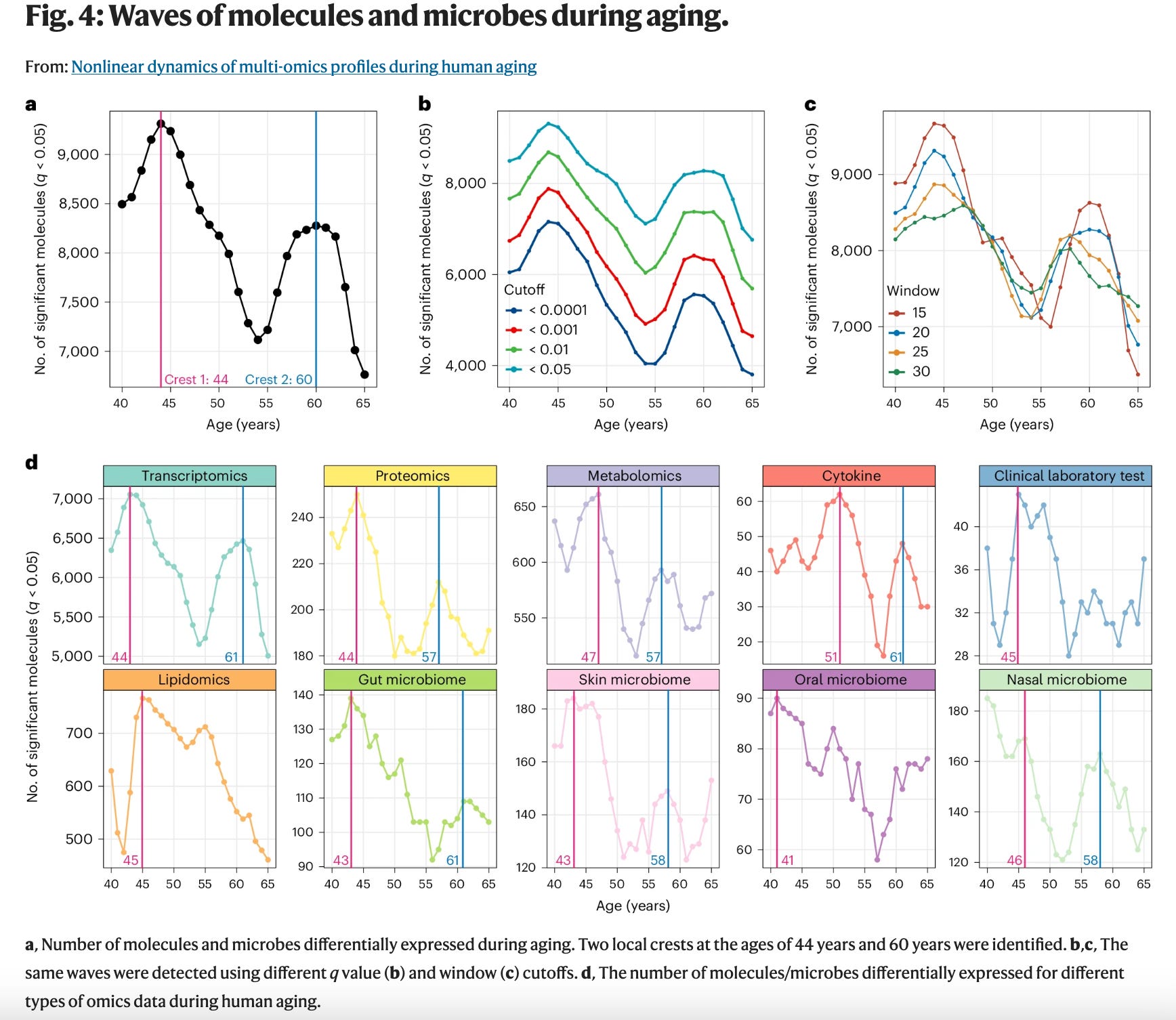
Age is fundamentally and inextricably linked to many of the chronic diseases that eventually kill us. There are some emerging age inflection points (44 and 60) that are associated with greater accumulation of disease. Can we reverse/halt/slow this process and is slowing/stopping aging the key to breaking through key asymptotes in progress on the biggest killers of our time?
The process of aging, and perhaps entropy, causes our bodies to go into a state of disorder compared to a normal past state. Our immune systems get exhausted (maybe recharged extra mitochondria can help), genetic defects don’t get self corrected via programmed cell death, harmful proteins build up in our brains., etc.
There seem to be phase transitions in chronic disease that are irreversible or only partially reversible. While there are investigations into how to reverse chronic conditions like diabetes, things don’t just reset back to normal. Extreme biohackers like Bryan Johnson are trying to reverse aging, through a mix of behavioral, nutritional and supplement interventions; however we don’t know if these steps actually change you back to normal or a more youthful state beyond “biological age” tests.
Can AI help us find how to stop and slow aging and chronic disease killers? Likely not directly, but maybe it will help us design better drugs for known modalities particularly for protein-based therapeutics like monoclonal antibodies. We are already seeing progress when it comes to AI/ML assisted early detection of cancer via “liquid” biopsies like GRAIL.
We will need new types of science to tackle these bigger questions: informed by complex systems / network science, decentralized, and/or augmented by AI (agents). These new paradigms could be the source of the next Nobel prizes in chemistry and medicine. I hope to address these and more topics in a future post.